
What is calcific tendonitis?
Calcific tendonitis is when calcium deposits form within the rotator cuff tendons of the shoulder. Most commonly occurring in the supraspinatus tendon.
What causes calcific tendonitis?
Calcific tendonitis occurs when, for no obvious reason, calcium deposits form within the rotator cuff tendons of your shoulder. The build-up of pressure can lead to intense shoulder pain that is unbearable.
The tissues (bursa) around the deposit also become inflamed. As with impingement syndrome, a bone spur and thickening of the ligament may develop over time causing narrowing of the space and further irritation of the tendon.
What problems does calcific tendonitis cause?
The symptoms from calcific tendonitis vary widely between individuals but most include a significant amount of pain and often some restriction in movement and function. If left for a significant period of time this can lead to a rotator cuff tear due to changes in the tendon from the deposit. Symptoms may include:
Pain
Pain is most commonly felt over the top and front of the shoulder joint and often in the upper part of the arm below the shoulder. Pain is often particularly severe when attempting to lift the arm overhead. Pain may be present at night, particularly if lying on the affected shoulder.
Limitation of movement
In some individuals movements can be so painful that it restricts the amount of movement a patient has.
Mechanical symptoms
There may be popping, clicking, crunching or grinding felt when moving the shoulder. Despite having a full range of movement there may be varying degrees of weakness.
Will I need any further investigations?
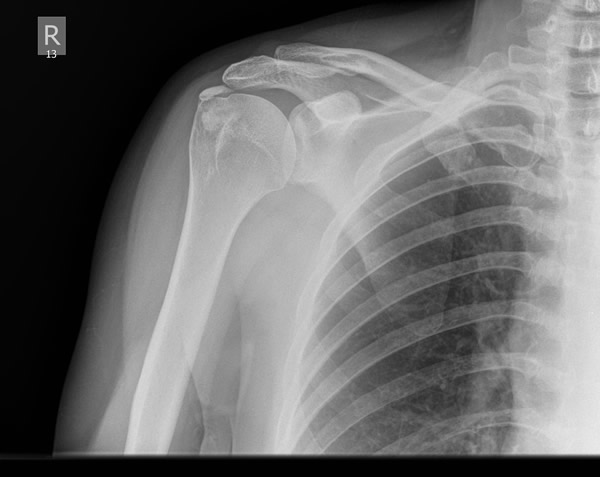
An X-ray of the shoulder is useful to rule out other causes of shoulder pain and the calcific deposits can often be seen on the X-ray. In some cases an ultrasound may be arranged if the status of the tendons is in doubt.
What can be done to treat calcific tendonitis?
Every patient with calcific tendonitis is different and responses to treatments vary between individuals. No single intervention works every time in every patient and deposits can recur in some patients. Your surgeon will help you decide which treatment is likely to be most effective.
Treatments can be divided into those involving surgery and those not involving surgery:
Non-surgical treatment:
Physiotherapy
A skilled physiotherapist advises with a variety of exercises to improve range of movement and strengthen the shoulder muscles.
Painkillers
Painkilling tablets, especially anti-inflammatory medication, often improve pain around the shoulder.
Injections
Injections of cortisone around the rotator cuff tendons often improve symptoms and can help to reduce the calcified deposit. These are most effective when combined with a course of physiotherapy. In many cases symptoms are permanently alleviated. If the effects of the injection wear off it can be repeated, although if injections only have a very brief effect, an alternative treatment may be more appropriate.
Surgical treatment:
Needle barbotage
The deposit can be released from the tendon using a needle. This can either be done using ultrasound guidance in theatre and flushed out with local anaesthetic or under direct vision with arthroscopy.
Subacromial decompression and direct evacuation
Most commonly performed through a keyhole (arthroscopy) under a general anaesthetic this procedure involves removing inflamed tissue from around the rotator cuff tendons (bursectomy) and shaving away bone from above the tendons (acromioplasty) increasing the space through which the tendons pass. The calcified deposit can then be removed from the tendon. In patients who have a large deposit and associated cuff tear it may be appropriate to repair the tendon at the same sitting.
What is the recovery after surgery?
You will have a sling to wear for comfort after the surgery that is usually discarded as soon as possible. You can safely use the shoulder within your comfort zone. Physiotherapy is essential after the operation, to encourage good movement, rehabilitate the muscles back to normal function and ensure you are making good progress. You will see a therapist prior to discharge from the hospital. You will be given painkillers to take home after surgery. You will be seen in clinic two weeks after surgery to check the wounds and assess your progress. There are no sutures to be removed. The pain will gradually settle and you will regain the movement in the shoulder over the next few weeks although it can take several months before you fully recover from the surgery.